
During the first year of the ARISE project, a landscape analysis was conducted to examine written documentation and existing data on RI systems in Africa, and to seek input from implementers and technical and development partners to improve understanding of the drivers of system performance. The landscape analysis report presents the findings of this initial investigation and the potential drivers of strong routine immunization system performance that emerged from this preliminary project phase.
To confirm the relevance of these drivers and better understand how they work in practice, ARISE conducted in-depth studies of selected districts in Ghana, Cameroon, and Ethiopia. These case studies explored not only which drivers are critical for improving district-level RI system performance, but also how they influence performance, the contextual factors impeding or promoting their effectiveness, and the relationship among different drivers. Drivers can operate on any stage of program cycle: Inputs, essential components, processes, or outcomes.
Through this case study approach with its mix of qualitative and quantitative methods, the ARISE partners undertook a consultative process of investigation to build on and contribute to the evidence base and to generate solutions to both old and new challenges. The articulation of strategies and steps to improve performance will involve a process of reflecting on the findings from these in-depth studies with global and local stakeholders.
Case Study Conceptual Framework
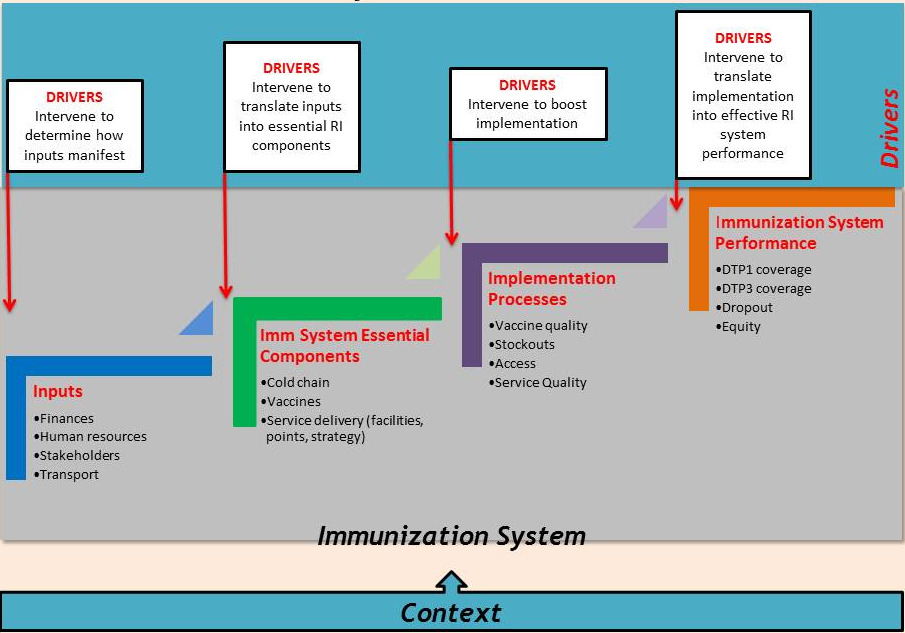 The ARISE team developed an analytical framework to guide the in-depth studies. The framework began with a logic model of the routine immunization system, then hypothesized that drivers of performance could intervene at the various and possibly multiple points along the pathway to RI performance. The in-depth case studies looked in detail at the district level to identify drivers of change, and describe and analyze how these drivers intervene with the immunization system to stimulate or accelerate improvements in RI coverage. ARISE also looked at how drivers behave and interact in different contexts.
The ARISE team developed an analytical framework to guide the in-depth studies. The framework began with a logic model of the routine immunization system, then hypothesized that drivers of performance could intervene at the various and possibly multiple points along the pathway to RI performance. The in-depth case studies looked in detail at the district level to identify drivers of change, and describe and analyze how these drivers intervene with the immunization system to stimulate or accelerate improvements in RI coverage. ARISE also looked at how drivers behave and interact in different contexts.
Context was defined as “those things that are outside the direct influence of the immunization system — including health system factors.”
In-Depth Country Case Study Methodology
In order to understand what was driving improvements in coverage, ARISE chose to conduct research in what ARISE called “positive change countries”, meaning those countries had had a positive increase in DTP3 coverage in the past 10 years (2000-2009). ARISE then focused within those countries on districts with recent positive change in DTP coverage. Ultimately, ARISE chose Ethiopia, Ghana, and Cameroon for study.
Districts within those countries were then selected if they had at least 65-70% coverage three years prior, and had reached over 80% DTP3 coverage in 2009-2010. Focusing on recent performance improvement experience allowed ARISE to reduce recall bias, and improve their chances of speaking with respondents who had been part of the performance improvement process. ARISE also chose, a priori, a “steady” district in each country that had similar baseline performance in 2007, but where coverage had not improved over the same period of time.
This study took a fundamentally different research approach than most immunization performance studies. ARISE purposely selected positive change districts so that they could study the following question: “What do you think has contributed to this rapid improvement in coverage?” Most analyses of immunization performance focus on the barriers to coverage improvement rather than the positive drivers of change. While challenges and barriers were not discounted, ARISE focused on their investigation and interviews on identifying the items that had worked well.
The experience of the positive change districts was then compared to the expereience of the “steady” district to see what was different. ARISE asked fundamental questions, such as:
- Were the items that worked well in the other districts present or absent in the steady district?
- If present, were they working as well?
- If they weren’t working as well, why?
ARISE asked these questions of a variety of respondents, to get a as close to a 360 degree perspective on immunization performance as possible. These interviews included national, regional/ zonal, district, sub-district, health center, health post, and community members. In all, ARISE spoke with about 300 individuals in 12 districts within the three case study countries.
In addition, ARISE conducted a rapid situation analysis of the Expanded Programme on Immunization (EPI) at the national and district level to determine whether there were any gaps or differences in the essential components of the EPI program, using a combination of available program data, record review, interviews, and observations.
However, coverage data proved to be problematic. In most situations, immunization performance could only be verified once the team had been in the district and examined the coverage data a very disaggregated level. While this did not invalidate the research approach used, it highlighted the importance of data quality and the difficulty relying on reported coverage data alone as a measure of RI system performance at the district level.

Two girls watch the ARISE team conduct interviews at the woreda health office in Ethiopia.